¶ Introduction
Breathing refers to the movement of air between the earth's atmosphere and the lungs. Breathing, or pulmonary ventilation as it is also known, is the process of ventilation which consists of two phases: inspiration whereby air enters the lungs, and expiration (or exhalation) whereby air exits the lungs.
Breathing can happen naturally or be supported by a mechanical ventilator, a device that moves air into and out of the lungs.
¶ Spontaneous Ventilation
Spontaneous ventilation refers to breathing caused by the body's own musculoskeletal system. The diaphragm muscle, located below the lungs, is the primary muscle used for breathing. Many other muscles in the body play a minor role, especially when coughing.
The volume inside the lungs increases when the diaphragm muscle contracts, causing the volume of the thoracic cavity to increase. The lungs return to a decreased volume when the diaphragm muscle relaxes. These changes in volume alter the pressure within the lungs, causing air to flow in or out.
Weakness of the diaphragm muscle reduces the amount that the thoracic cavity can increase in volume, which correspondingly reduces the amount of air that will flow into the lungs. Mild or moderate decreases in flow volume are tolerable, however, more significant decreases will require ventilation support.
Side Note: Oxygen therapy
A lack of airflow into the lungs during inspiration will also cause a lack of airflow out of the lungs during expiration. Together, these two phenomena cause blood oxygen levels to decrease, and blood carbon dioxide levels to increase. Therefore, oxygen therapy would not benefit someone in this condition, as the oxygen therapy does not in any way cause the excess carbon dioxide in the blood to be removed.
An individual with ALS should not seek nor receive oxygen therapy in most circumstances.
¶ Mechanical Ventilation
Mechanical ventilation refers to ventilation that is supported by a mechanical device. There are two types of ventilators: non-invasive, and invasive.
Mechanical ventilators are typically used to assist with natural ventilation, by relieving the diaphragm muscle of at least some of the load. At the extreme, they are able to entirely take over the task of providing adequate ventilation.
Mechanical ventilators cause inspiration by using pressures higher than the surrounding atmospheric pressure to force air into the lungs. Expiration is caused by reducing the pressure somewhat; the lungs return to a smaller volume, which causes air to flow back out of them.
Side Note: CPAP machines
Continuous positive airway pressure (CPAP) machines are not considered to be mechanical ventilators as they do not regulate the flow of air into and out of the lungs.
As the name suggests, a CPAP machine creates and maintains a continuously positive pressure in the airway, which is used to help keep the airway open. CPAP machines are thus useful for treatment of obstructive sleep apnea, where the airway becomes blocked during sleep.
CPAP machines are not associated with managing the symptoms of ALS; some individuals with ALS may use them if they suffer from obstructive sleep apnea, and do not yet require the use of a true mechanical ventilator.
¶ Non-Invasive Ventilation
Non-invasive ventilation refers to mechanical ventilators which do not enter the body. Removable masks and nasal fittings are used to deliver air into the airway. With ALS, not in base of ventilation is accomplished with the use of a bi-Level ventilator.
Bi-level ventilators, also known by the trade name BiPAP®, are non-invasive ventilators that alternate between a high and low pressure to facilitate breathing.

ResMed Stellar 150 bi-level ventilator with humidifier.
Article: Bi-Level Ventilators ›
¶ Invasive Ventilation
Invasive ventilation refers to mechanical ventilators that enter the body. Two different methods are used to enter the airway: intubation, which involves placement of a removable tube down the throat, and tracheostomy, a surgical procedure where a hole is placed at the base of the neck and the tube is inserted at that point.
¶ Respiratory Therapy
A core component of ALS care is management of breathing symptoms. A pulmonologist, also known as a respirologist, will periodically order tests to measure independent breathing function. Mechanical ventilation will be introduced when independent breathing function measurements have shown inadequate ability.
Non-invasive ventilation is typically the first step in respiratory therapy. At first, it may only be used a few hours per day, or overnight. Usage will increase as respiratory difficulties continue to advance.
Invasive ventilation, typically in the form of tracheostomy, is used when non-invasive ventilation is no longer adequate.
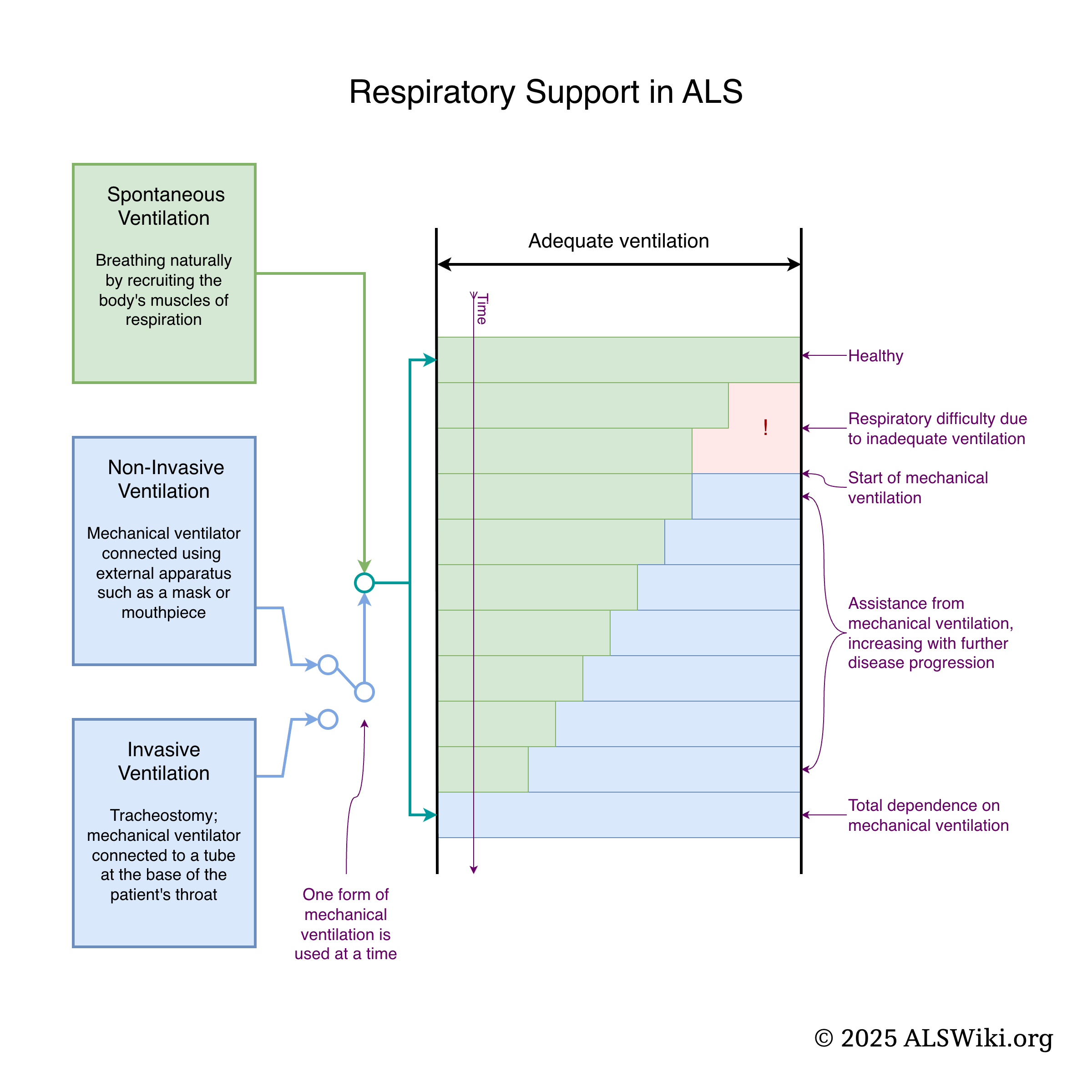
Infographic: Respiratory Support in ALS. Click to expand.
Side note: respiratory muscle trainers
A respiratory muscle trainer is a mechanical device that is used to strength train breathing muscles by moderately restricting airflow.
Although pulmonologists rarely suggest respiratory muscle trainers for people with ALS, a 2023 study reported modest benefits in certain breathing functions when used in the disease’s early stages. However, the overall rate of disease progression and the time until patients required non-invasive ventilation remained unchanged.[1].
Respiratory muscle trainers are available without a prescription, however, they should only be used when advised to do so by a qualified physician.
¶ Reflexes
¶ Coughing
🚧
¶ Sneezing
🚧
¶ Yawning
🚧
¶ See Also
Breathing
Article Collection
General
- Breathing – Introduction to breathing
- Glossopharyngeal breathing – a.k.a. "frog breathing"
- Tracheostomy – Neck tube inserted for breathing
Therapy Devices
- Bi-Level Ventilators – a.k.a. BiPAP®
- Lung Volume Recruitment Bags – links to: Lung Volume Recruitment
- Mechanical Insufflator-Exsufflators – a.k.a. Cough Assist
- Mouthpiece Ventilators
Tasks
¶ References
- Emily K Plowman, Lauren T Gray, Jennifer Chapin, Amber Anderson, Terrie Vasilopoulos, Clifton Gooch, Tuan Vu, James P Wymer, "Respiratory Strength Training in Amyotrophic Lateral Sclerosis: A Double-Blind, Randomized, Multicenter, Sham-Controlled Trial - PubMed", PubMed, Retrieved 2025-12-03