¶ Introduction
Main floor living refers to adapting a typical multistorey home to be suited for an ALS patient to live on only the main floor.
¶ Purpose and Benefits
Living on the main floor provides an alternative to moving into a new home or care facility when using stairs is no longer feasible. Other key benefits include:
- Avoids the costs associated with moving
- Minimizes or eliminates the need for renovations, which may be costly and time-consuming
- Allows continued use of existing adaptive equipment and home modifications
- Preserves a familiar lifestyle, both within and outside the home
- Maintains access to an existing care team
¶ Considerations
This article makes the assumption that the destination room on the main floor is the living room. Certainly, any other suitable on the main floor could be occupied instead.
The room should be evaluated thoroughly before making plans to move into it. The following factors should be considered:
- Room size and layout
- Flooring
- Discoverability
- Communication
- Noise
- Privacy
- Toileting and bathing
¶ Room size and layout
The destination room must be large enough to accommodate all necessary items while still leaving adequate space for safe transfers and for caregivers to carry out their duties.
The dimensions of both the room and all items to be placed in it should be accurately measured. It's worthwhile to create the intended layout using specialized room design software or drawing tools that support adding precise dimensions. This helps ensure everything fits properly.
Floor space is valuable, so it's best to mount items on the wall whenever possible. For example, wall-mounting a television can free up floor space. Other space-saving options include using wall-mounted lamps and replacing floor-standing drawers with shelving.
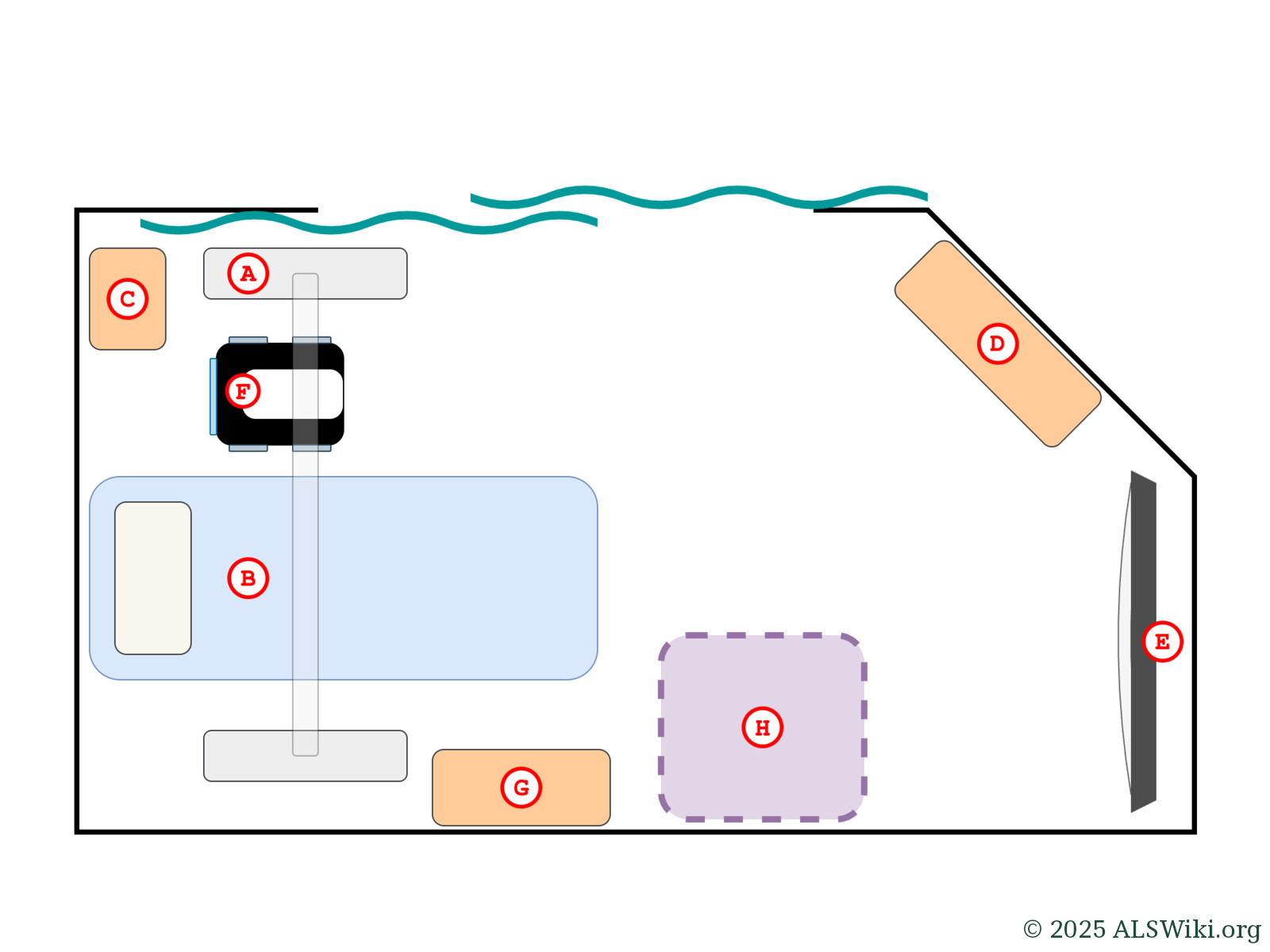
Example floor layout.
a. Freestanding ceiling track lift; feet and tracking
b. Bed
c. Small table
d. Large table
e. Television
f. Commode chair, positioned for use
g. Storage cabinet
h. Recliner, or wheelchair parking
Ceiling height is an important factor when using ceiling lifts. Floor lifts are less demanding, as the hanger bar typically mounts very close to the boom of the lift, meaning that it can go very high before coming in contact with the ceiling.
¶ Flooring
The flooring in the room must be suited to performing safe transfers. Carpet, unless it is extremely shallow pile, is not acceptable. Even then, shallow carpet is prone to getting dirty and trapping smells.
The floor should be in good condition and free of large cracks, holes, or other damage.
¶ Discoverability
It must be clear to visiting caregivers and emergency services that there is a person living in a room that is not typically occupied. Markings of some sort, or some other system should be in place to make it obvious for such people.
¶ Communication
The patient will be alone in the living room in most cases. Other members of the household typically remain in designated bedrooms. As such, it must be possible for the patient to communicate with others in the home in case of any need.
¶ Noise
The room of choice on the main floor may be near a kitchen, entryways, or large windows, which can all be sources of noise.
Reducing the effects of noise is difficult; any open archway or wall opening would need to be filled in. Windows would need to be replaced with models designed to block sound.
Most conventional curtains have an STC (Sound Transmission Class) of approximately zero, meaning that they block almost no sound.
Noise can have a significant impact on sleep quality, and the ability to communicate with others in the home. Noise from a running faucet or range hood in a kitchen can be strong enough to drown out voice dictation being used on a computer or smartphone.
¶ Privacy
¶ Archways
Rooms that have very large archways with no doors must be concealable for the patient to have privacy. At the same time, reasonable airflow must be maintained.
Curtains are typically used for this purpose; their placement can be optimized in such a way as to provide privacy and decent airflow.
¶ Wall openings
A wall opening (or interior window) is an opening on an interior wall to the living room. These can be covered with curtains, or filled in with a large piece of foam.
Foam has the advantage of providing some sound isolation, along with blocking airflow that may cause the curtains to move when people walk by or when an exterior door or window is opened. The foam can be covered with a curtain, a tapestry, or a large poster.
¶ Windows
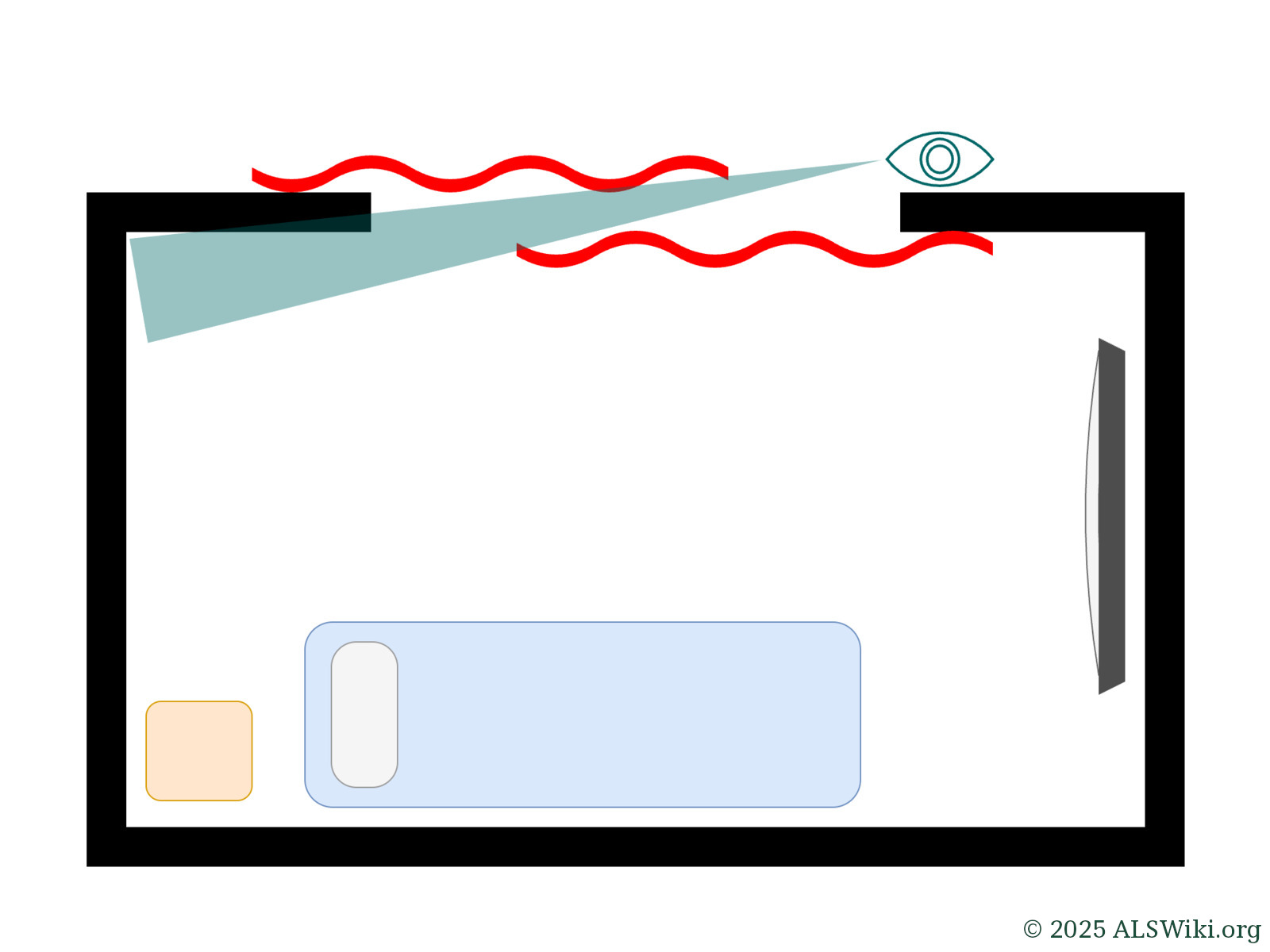
Some living rooms have large windows which face the street. Privacy film can be applied to the windows so that people cannot see in. A portion of the upper section of the windows may be left uncovered. However, at night, people outside may be able to see the silhouettes of what is going on in the room. This may be embarrassing for the patient if they are receiving a bath or toileting.
Any effort to conceal the living room from being viewed outdoors should be verified at night, with all lighting in the room turned on.
¶ Sound
Privacy in terms of sound is difficult to achieve in most living rooms. Curtains do not provide any meaningful sound isolation, unless they are specifically designed to do so. Even still, sound isolating curtains do not work if they have large gaps or are left open.
¶ Toileting and bathing
The main floor of the home may not have a bathroom that is accessible, or any bathroom at all.
Toileting can be accomplished by using a commode chair. Commode chairs with wheels are easy to remove in order to recover precious floor space or when entertaining guests.

A wheeled commode chair is ideal for toileting in a living room since it can be moved elsewhere when not in use.
Bathing can be accomplished by sponge bathing in bed, or by using a portable shower setup.
¶ Room Adaptations
¶ Electrical outlets
Electrical outlets in the living room should be inspected. Essential equipment such as ventilators will be plugged into these outlets, so they must be in good condition. Any that are found to be damaged or not able to firmly hold a plug should be replaced.
Electrical outlets which are near areas of the room where sponge bathing or use of a commode chair is to take place should be covered or removed.
¶ Lighting
Ceiling lift tracking and positioning of items such as a hospital bed or commode chair may affect lighting in the room. Areas where the patient will be receiving care, such as on the bed, should be suitably well lit, especially when a caregiver is standing at the side of the bed.
Some living rooms have no overhead lighting at all. When possible, adequate lighting should be achieved by installation of overhead or wall-mounted lighting, to minimize use of floor space.
¶ Curtains
Curtains are the most common solution to covering an archway to a living room. Another alternative is to fill the archway with a wall, and install a door. Doing so may have airflow implications, depending on the ventilation system in the home.
Conventional curtains that rest on a curtain rod are suitable for most needs. A wand should be installed so that opening and closing them can be done without having to pull down on them.
Curtain rod brackets should be screwed directly into wall studs. Brackets that are screwed into the drywall with anchors are prone to tearing out with frequent use.
A single curtain panel should be used to cover the archway whenever possible. Using two separate panels, one on each side, can result in a gap where they meet, compromising privacy. While placing one panel on the opposite side of the archway can eliminate this central gap, it may still leave a small portion of the living room visible through the opening, as the curtain spans from opposite sides and doesn't fully block the view when looked at from an angle.
Installing curtains on both sides of the archway with substantial overlap allows for easy entry and exit without needing to draw them open. However, this setup does leave part of the room visible from the outside.
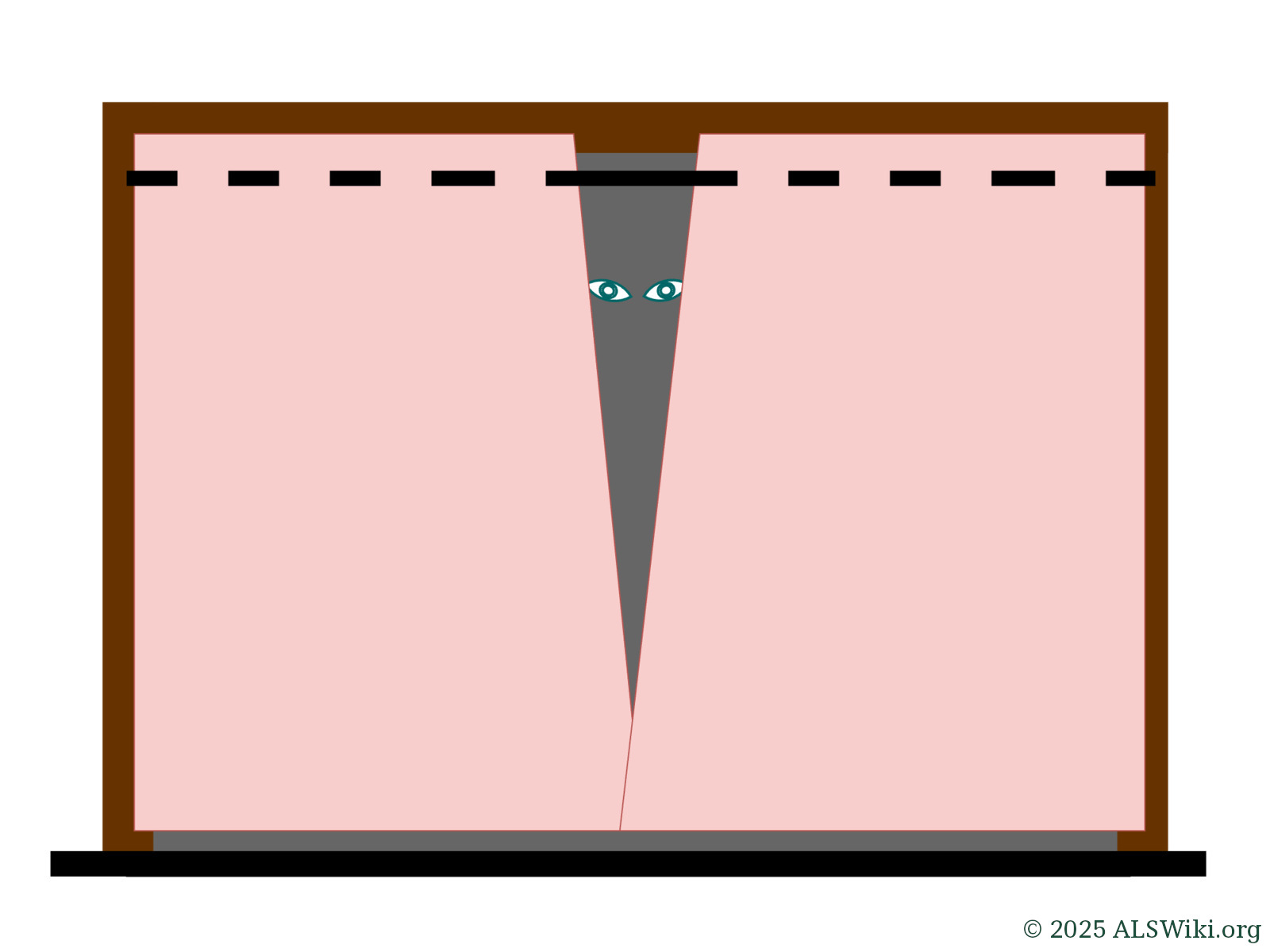
Separate panels that meet in the middle can be difficult to close fully at the top. This can leave a sizeable gap, allowing people to see inside the room.
¶ Ceiling lift tracking
A ceiling lift is ideal for transfers in confined spaces such as a living room. The joists in the ceiling must be inspected to ensure that they are suited to the mounting of a ceiling lift track. If they are not, a ceiling lift with supportive columns may be used instead.
¶ See Also
¶ Adaptive Equipment
¶ Living with ALS
- In-Home Communication Call bells • Smart doorbells • Communication services
- Stay-or-Move Decision Factors in deciding whether to stay or move
- Toileting